Confused about health numbers, here’s some
help to sort them out:
1. Cholesterol as a marker of CVD (cardiovascular disease) isn’t a helpful indicator!
** 44 randomised controlled trials (RCTs) of drug or dietary interventions to lower LDL-C in the primary and secondary prevention literature, which show no benefit on mortality[8]. Most of these trials did not reduce CVD events and several reported substantial harm. Yet, these studies have not received much publicity.
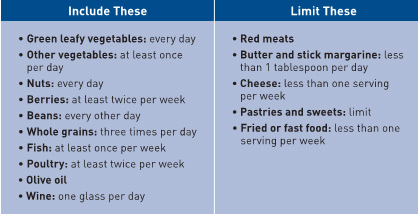
2. Calories are not the enemy, where calories come from matters most.
*** Current thinking about obesity and related diseases holds that quantifying calories is the principal concern and target for intervention. The basis for this directive is that consumed calories, regardless of their sources, are equivalent; i.e. ‘a calorie is a calorie’. Rather, a focus on the sources of those calories consumed (i.e. processed versus real food) and on the metabolic changes that result from consuming foods of different types needs to be addressed[26]. In particular, calorie-focused thinking is inherently biased against high-fat foods, many of which appear to be protective against obesity and the diseases of metabolic syndrome, and supportive of refined starch and sugar replacements, which are clearly detrimental, and exclusive of their calories and effects on weight gain[27],[28].
3. Monitor INSULIN RESISTANCE numbers to get a more accurate picture into chronic disease risk. Fasting blood glucose above 100 is problematic (below 85 is best) & A1c below 5.7% is the target.
People with insulin sensitivity have the lowest disease risk of all!
https://www.pharmaceutical-journal.com/news-and-analysis/opinion/insight/the-cholesterol-and-calorie-hypotheses-are-both-dead-it-is-time-to-focus-on-the-real-culprit-insulin-resistance/20203046.article
help to sort them out:
1. Cholesterol as a marker of CVD (cardiovascular disease) isn’t a helpful indicator!
** 44 randomised controlled trials (RCTs) of drug or dietary interventions to lower LDL-C in the primary and secondary prevention literature, which show no benefit on mortality[8]. Most of these trials did not reduce CVD events and several reported substantial harm. Yet, these studies have not received much publicity.
2. Calories are not the enemy, where calories come from matters most.
*** Current thinking about obesity and related diseases holds that quantifying calories is the principal concern and target for intervention. The basis for this directive is that consumed calories, regardless of their sources, are equivalent; i.e. ‘a calorie is a calorie’. Rather, a focus on the sources of those calories consumed (i.e. processed versus real food) and on the metabolic changes that result from consuming foods of different types needs to be addressed[26]. In particular, calorie-focused thinking is inherently biased against high-fat foods, many of which appear to be protective against obesity and the diseases of metabolic syndrome, and supportive of refined starch and sugar replacements, which are clearly detrimental, and exclusive of their calories and effects on weight gain[27],[28].
3. Monitor INSULIN RESISTANCE numbers to get a more accurate picture into chronic disease risk. Fasting blood glucose above 100 is problematic (below 85 is best) & A1c below 5.7% is the target.
People with insulin sensitivity have the lowest disease risk of all!
https://www.pharmaceutical-journal.com/news-and-analysis/opinion/insight/the-cholesterol-and-calorie-hypotheses-are-both-dead-it-is-time-to-focus-on-the-real-culprit-insulin-resistance/20203046.article







 RSS Feed
RSS Feed
